
From 1Polio Australia Incorporated, 2Discipline of Exercise and Sports Science, School of Science and Technology, University of New England and 3Adelaide Medical School, Faculty of Health and Medical Sciences, The University of Adelaide, Australia.
Objective: To evaluate and assess the effectiveness of muscle strengthening and cardiovascular interventions in improving outcomes in poliomyelitis (polio) survivors.
Data sources: A systematic literature search was conducted in Medline, PubMed, CINAHL, PsychINFO, Web of Science, and Google Scholar for experimental and observational studies.
Study selection and extraction: Screening, data-extraction, risk of bias and quality assessment were carried out independently by the authors. The quality appraisal and risk of bias were assessed using the Downs and Black Checklist. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was followed to increase clarity of reporting.
Data synthesis: A total of 21 studies that met all the inclusion criteria were subjected to statistical analyses according to intervention (muscle strengthening or cardiovascular fitness). A random-effects meta-analysis showed a statistically significant effect for the exercise interventions favouring improvement in outcomes according to the International Classification of Functioning, Disability and Health (ICF).
Conclusion: This review provides further insight into the effects associated with muscle strengthening and cardiovascular interventions among polio survivors, and helps to further identify the current state of research in this area. Future research is needed, focusing on individualized approaches to exercise with polio survivors and specific exercise prescription recommendations, based on established frameworks, such as the ICF.
Key words: post-polio syndrome; International Classification of Functioning, Disability and Health framework; exercise-based intervention; rehabilitation.
Accepted Mar 25, 2021; Epub ahead of print Apr 19, 2021.
J Rehabil Med 2021; 53: jrm00184
Correspondence address: Dr Timothy Lathlean, Discipline of Exercise and Sports Science, School of Science and Technology, University of New England, Armidale, Australia. E-mail: Tim.lathlean@une.edu.au
Doi: 10.2340/16501977-2832
Polio survivors are an ageing population and prone to functional decline. Multiple age-related diseases affect this population, in addition to Late Effects of Polio (LEoP). Exercise plays an important role in improving strength and overall cardiovascular fitness in these individuals, and clinicians face challenges when advising polio survivors on the optimal level of exercise to avoid producing pain and/or fatigue. Improvements in strength and cardiovascular fitness have the potential to translate into activities of daily living within this cohort. To our knowledge, this is the first systematic review and meta-analysis using a broad approach (i.e. including both experimental and observational studies) to capture and summarize the research to date regarding the role of muscle strengthening and aerobic conditioning exercise in polio survivors. This review provides valuable information for clinicians, which will help enable the development of specific exercise prescription appropriate to this population.
Poliomyelitis (polio) is a highly infectious, viral disease that affects the nervous system and can cause total paralysis (1). Based on published records, the World Health Organization (WHO) estimates there are 20 million polio survivors worldwide (1). Although outbreaks of polio have reduced significantly as a result of vaccination, 15–80% of all polio survivors develop post-polio conditions (2). Post-polio syndrome (PPS) is a clinical diagnosis in which symptoms may become apparent 15–30 years after exposure to polio (3, 4). PPS is characterized by progressive or new muscle weakness, generalized fatigue, muscle atrophy and pain (4, 5). Internationally, the cluster of signs and symptoms that include PPS features and additional biomechanical symptoms is referred to as Late Effects of Polio (LEoP) (6).
PPS can lead to significant disability, including inability to work, loss of mobility and loss of independence (4). Many individuals with PPS report being inactive, due to weakness and fatigue; symptoms that are perceived to worsen with activity (4). Reduced physical activity associated with muscle atrophy and deconditioning can then potentiate further fatigue and weakness and be linked with reduced muscle capacity and cardiovascular fitness, probably contributing to higher comorbidity rates and potential hospitalization (7). Aerobic fitness intervention modalities, such as walking, cycling, arm ergometry and water-based exercise, have been shown to be effective in attenuating decline in function in patients with PPS (8, 9). Furthermore, muscle strengthening training can also increase functional capacities in individuals with PPS (5), with previous research reporting improvements in isometric and isokinetic strength in individuals with PPS (4).
A recent systematic review initially raised concerns that polio survivors might overload weak muscles during exercise, causing an increase in symptoms, such as pain, fatigue and weakness (5). Despite this common concern, based on the methods used in this review, limited evidence was found to substantiate this (5). Earlier, a 2008 meta-analysis, limited by the number and quality of included studies, showed some cardiovascular outcomes could be improved in polio survivors, but apparent positive effects of strengthening were not significant (10). Such conflicting recommendations may cause clinicians and polio survivors to experience concerns about further risk of adverse outcomes when considering whether to pursue exercise programmes (8). The management of PPS symptoms is essential for maintaining quality of life and independence (11, 12). The benefits of exercise for those with non-communicable diseases comparable to PPS include improvements in productivity and wellbeing, and reduction in health system expenditure, further identified in a recent study focused around the role of the clinical exercise physiologist (13).
Clinicians can experience uncertainty when advising polio survivors on exercise, as divergent results and recommendations exist (10, 14). Limited modes of exercise have been studied in the literature with regard to this population, but aspects of exercise have been sufficiently tested to prompt this review. This systematic review and meta-analysis aims to summarize current knowledge of the effectiveness of muscle strengthening and cardiovascular interventions (and/or mixed interventions including both) in improving outcomes in polio survivors. The main hypothesis of this study is that these exercise interventions will improve outcomes in polio survivors above and beyond usual practice.
Search strategy
The following computerized databases were searched for articles published from their respective inception dates to 20 February 2020, inclusive: Medline, PubMed, CINAHL, PsycINFO, Web of Science, and Google Scholar. Search terms were mapped to MeSH terms, or subject headings and synonyms were grouped together using Boolean operators. A range of search terms were used to identify the population, exercise interventions, and outcomes (see Table SI). Both experimental (e.g. randomized controlled trials; RCTs) and observational (e.g. cohort studies) study designs were included in the search strategy and inclusion criteria. Results of the database searches were downloaded into Endnote X8 (Clarivate, Philadelphia, US) and duplicate papers were excluded. One author (AR) screened citation titles and abstracts for potentially relevant titles and abstracts. Article full-text versions were then screened (AR and TL). Disagreements were resolved by consensus with the 2 remaining authors. Reference lists of all studies assessed against the eligibility criteria were also screened for additional literature.
Inclusion and exclusion criteria
Articles were included if: (i) the study targeted a sample of participants experiencing LEoP or PPS following a period of stable neurological function after 15 years; (ii) the focus was on original research; (iii) an exercise intervention was used; and (iv) publication was after 1980. Studies were excluded if they were: (i) conference or poster presentations; (ii) not original research; or (iii) not in English. Studies were not restricted by study design.
Quality assessment and risk of bias
Two independent reviewers (AR and TL) assessed the quality of the included studies using Downs and Black checklist (15) (Table SII). The checklist consists of 27 questions addressing study reporting, external validity, internal validity (bias, confounding) and power. The quality index of the checklist has high criterion validity (r = 0.90), high internal consistency (KR-20 = 0.89), test-retest (r = 0.88) and inter-rater (r = 0.75) reliability. For dimension reduction purposes, these items were reduced to 17 questions, with each question coded as either “yes”, “no”, or “undetermined”. The sum of each “yes”’ response contributed to the overall quality score, where higher scores indicate greater methodological quality. High-quality studies were categorised as 85–100%, moderate quality studies as 60–84%, and low quality as less than 59% (15). Two authors (AR and TL) rated each article independently. All disagreements (n = 15; 4% of all questions) were discussed at a consensus meeting and appropriate ratings decided on by the remaining authors.
Level of evidence
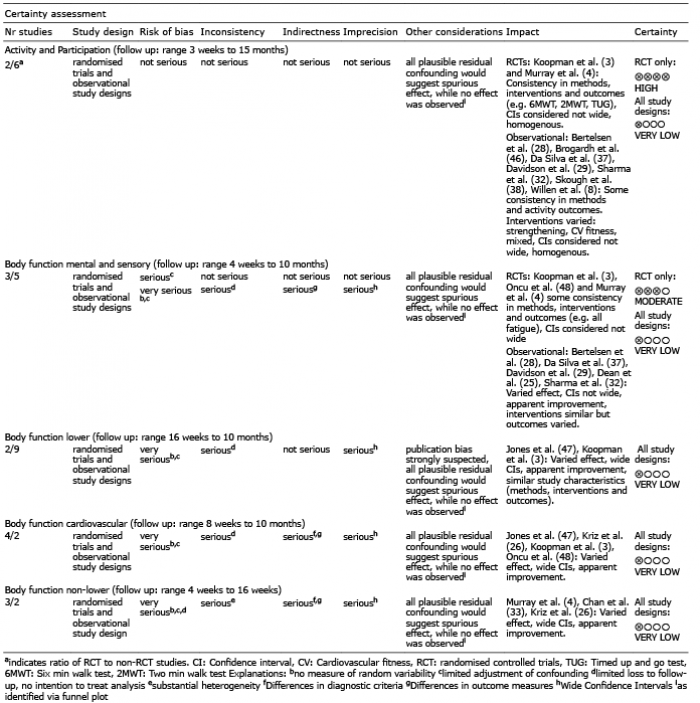
According to the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework (16), the quality of evidence in this review can be utilised to help make recommendations to clinicians and polio survivors. Hence, based on risk of bias, inconsistency, indirectness, imprecision and other considerations, a summary of findings table was produced (Table I), highlighting overall certainty as well as the clinical importance of each key domain outcome.
Table I. Summary of findings based on outcome domains and study design
Data extraction
The following data were extracted from included studies: author, study population, diagnosis criteria used, study design, follow-up time, type of exercise intervention, outcome measures, statistical analysis, and effects of the intervention. The International Classification of Functioning, Disability and Health (ICF) codes provide a framework for understanding the interactions of environment, conditions and personal factors on influencing body function and structure, activities and participation (17). Table SIII outlines second-level domain coding of the ICF for study outcome measures. Based on a proposed ICF Core Set for PPS (17), outcomes were grouped into the following ICF domains: body function component (1) muscular; (2) cardiovascular; (3) mental and sensory; and as a dual component domain (4) activity and participation.
As outlined in Table SIII, the muscular function domain contains outcome measures such as isometric and dynamic strength, the cardiovascular domain contains outcome measures such as peak oxygen uptake, heart rate, blood pressure, and aerobic capacity (VO2) and mental and sensory domain contains pain and fatigue. The activity and participation domain contains outcome measures (from activities) such as 6-min walk test, 6-min arm test, Timed Up and Go test, 10-metre walk test, 2-min walk test, and (from participation) such as daily physical activity level scale for people with disabilities, Short-Form 36 (SF-36), physical component summary, mental component summary.
Data analysis
Following data extraction, effect sizes and their corresponding 95% confidence intervals (95% CI) were derived for each individual outcome. In the event multiple outcomes denoted a given ICF domain or component, a representative effect size was calculated by pooling the effect size of each outcome using Comprehensive Meta-analysis v3 (BioStat, Englewood, NJ USA). Data were sub-grouped into the respective interventions used (aerobic fitness, mixed, and muscle strengthening) and meta-analyses were completed on the combined body function domain, and each of its underlying components (lower limb, non-lower limb, cardiovascular, and mental and sensory), and a collated activity and participation domain. For all analyses, a generic inverse variance, random effects model was used. This model was adopted due to the anticipated differences among studies (study duration, outcome measures, and/or post-polio condition severity). Effect sizes were reported as Hedges g, with the magnitude of the effect defined using standardized conventions, where small, moderate, and large are represented by values of 0.20, 0.50, and 0.80, respectively (18). Significance was investigated through the use of p-values, where the alpha was set at ≤ 0.05. Heterogeneity was evaluated using Cochran’s Q, where the alpha was set at ≤ 0.10. In the event significance was reported, the I2 statistic was then explored to define the magnitude of heterogeneity about the result, where 0–40, 30–60, 50–90, and 75+ were suggestive of low, moderate, substantial, and considerable heterogeneity, respectively (19). Leave-one-out sensitivity analyses were conducted when statistical heterogeneity was reported. In order to investigate the effects of intervention duration on the domains and/or components of the ICF, meta-regression was performed at the study level using a random-effects model. Publication bias was also investigated statistically through the Begg and Mazumdar’s rank correlation test and Eggers linear regression model, which were applied to each component and the overall analyses. If publication bias was detected, Duval and Tweedie’s trim and fill correction was applied and the resultant Hedges g and associated 95% CI were explored. Given the software used for these analyses the L0 estimator was used to formulate the correction. GRADEPro GDT (20) (McMaster University, Hamilton, Ontario, Canada) was used to develop a summary of findings table consistent with the GRADE handbook (16).
Systematic search and study quality
Fig. 1 shows the flow diagram of the systematic search, consistent with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (21). The search strategy produced 2,644 citations from 6 databases. Following the removal of duplicates, 2,327 studies remained. After title and abstract screening, 48 studies were then assessed against the eligibility criteria, where 21 citations were then included and assessed for study quality, with the quality assessment scores ranging from 53% to 88%. The mean (standard deviation (SD)) score of study quality was found to be 72.5 (10.5) %. Individual scores for each study are also shown in Table SIII. Of those studies satisfying study quality, there were 2 instances where more than one article was based on the same sample (3, 9, 22, 23), with the latter also examining both isometric and isokinetic exercise. Hence, the latter study in each circumstance of overlapping samples was removed from the analysis. Furthermore, one study (24) was divided into 2 cohorts to reflect 2 different intervention contexts (e.g. hospital-based compared with home-based).
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (21) flow diagram outlining the identification and inclusion process for the quantitative review. PPS: post-polio syndrome.
Study descriptions
Of the studies included in this systematic review, 7 were RCTs, 4 were controlled trials, 7 were longitudinal studies, with the remaining 3 either cross-sectional, case-crossover or case-control design. Study duration ranged from 5 to 32 weeks, with sample size ranging from 5 to 68 participants with post-polio conditions. Of the included studies, 5 focused on aerobic fitness interventions (4, 24–27), 7 on mixed interventions (aerobic fitness and muscular strengthening/functional activities) (3, 9, 28–32) and 9 on muscular strengthening interventions (22, 23, 33–39). Table II summarizes the study population, sample size, study design, follow-up time, type of exercise intervention, outcome measures and statistical analysis and associations.
Table II. Experimental study designs according to study design and intervention type (cardiovascular fitness, mixed intervention methods and muscle strengthening)
Table II. Cont.
Table II. Cont.
Table II. Cont.
Meta-analyses: the effect of exercise interventions
Fig. 2 shows the separate and combined effects of exercise interventions on the body function domain. When collated in this manner, aerobic, mixed and strengthening interventions were shown to have a small-to-moderate effect (g ranging from 0.217 to 0.506; all p < 0.01); however, heterogeneity ranged from substantial to considerable (all p < 0.01; I2 ranging from 70% to 83%). The overall effect on the body function domain indicated exercise interventions have a small positive effect (g = 0.298; 95% CI = 0.191–0.406; p < 0.01); however, substantial to considerable heterogeneity was evident (Q(22) = 106.499; p < 0.01; I2 = 79%). To determine the robustness of these findings, a leave-one-out sensitivity analysis was completed and the output reported in Table SV(A–D). Table SVI (A shows a sensitivity analysis where both (9, 22) were removed from the analysis, as participants used in these studies may have been repeated. For the combined body function domain, the results of this analysis were comparable to the main analysis, where all interventions and the combined overall effect were significant (all p ≤ 0.01) and the same effect size ranges were maintained (g ranging from 0.237 to 0.506). All data were substantial to considerably heterogeneous (all p ≤ 0.01; I2 ranging from 73% to 83%).
Fig. 2. Forest plot of the combined body function domains of the International Classification of Functioning, Disability and Health (ICF) disability framework. Studies are divided into their respective intervention types (aerobic fitness, mixed, and strengthening exercise).
Table III shows the meta-analysis summaries for each of the examined components and/or domains of the ICF. Within the body function domain, when all interventions were combined, small-to-moderate effects were identified in the lower limb, non-lower limb, and mental and sensory components (g ranging from 0.178 to 0.463; all p < 0.01). Only the cardiovascular component was not significant (g = 0.114; 95% CI = –0.034 to 0.262; p = 0.13). Significant heterogeneity was present for each of the components within the body function domain and ranged from moderate to considerable (all p ≤ 0.01; I2 ranging from 54% to 78%). Output from the leave-one-out sensitivity analysis is shown in Table SV(E, H, I and L).
Table III. Meta-analysis output for each of the components examined in the International Classification of Functioning, Disability and Health. Positive direction denotes the respective intervention mode having a beneficial effect on the respective domain and/ or component.
Aerobic interventions within the body function domain were shown to produce significant small-to-large effects in the non-lower limb, cardiovascular, and mental and sensory components (g ranging from 0.260 to 0.733; all p ≤ 0.01). Data were homogenous for the finding in the non-lower limb (Q(1) = 0.151; p = 0.70; I2 = 0%), while substantial heterogeneity was found within the cardiovascular and mental and sensory components (both p = 0.01; I2 ≥ 68%). The effect of aerobic interventions on the lower limb component was not explored, due to an insufficient number of
studies (n = 1). Output from the leave-one-out sensitivi-ty analysis is shown in Table SV(J and M).
For mixed interventions within the body function domain, small improvements were found for the lower limb and mental and sensory components (g = 0.140 and 0.197 respectively; both p ≤ 0.05), while the cardiovascular component was not significant (g = 0.007; 95% CI = –0.169 to 0.183; p = 0.94). Data for mixed interventions were not interpreted for the non-lower limb component due to an insufficient number of studies (n = 1). For each of these findings, heterogeneity was not significant (all p ≥ 0.20; I2 ≤ 35%). Output from the leave-one-out sensitivity analysis is shown in Table SV(F and N). Removal of (9) resulted in significance being lost for mixed interventions in the lower limb component (g = 0.127; 95% CI = –0.028 to 0.281; p = 0.11), while there were insufficient study numbers to interpret the cardiovascular component (g = –0.092; 95% CI = –0.299 to 0.115; p = 0.38), shown in Table SVI.
For strengthening interventions, a positive small-to-moderate effect was found for the lower limb and mental and sensory components (g = 0.232 and 0.356 respec-tively; both p ≤ 0.05). Although substantial heterogeneity was present for the lower limb (Q(6) = 18.614; p < 0.01; I2 = 68%), data were considered homogenous for the mental and sensory component (Q(1) = 0.398; p = 0.53; I2 = 0%). The main effect here appears to be between muscle strengthening exercise and fatigue, as fatigue measures accounted for 36% (13 of 36) compared with pain measures (19%) of the mental and sensory measures reported in the included studies. Within the non-lower limb component, muscle strengthening did not produce a significant effect (g = 0.337; 95% CI = –0.341 to 1.015; p = 0.33), but substantial to considerable heterogeneity was also present (Q(1) = 5.379; p = 0.02; I2 = 81%). Output from the leave-one-out sensitivity analysis is shown in Table SV(G and K). Removal of (22) resulted in a loss of significance for muscle strengthening in the lower limb component (g = 0.235; 95% CI = –0.049 to 0.519; p = 0.10; Table SVI (B)), and data were substantially heterogeneous (Q(5) = 17.887; p < 0.01; I2 = 72%). This study did not contribute to the remaining components.
For the combined activity and participation domain, exercise interventions produced a small positive effect (g = 0.143; 95% CI = 0.088–0.198; p < 0.01). A small positive effect was also found for mixed interventions (g = 0.145; 95% CI = 0.086–0.204; p < 0.01). The aerobic and strengthening interventions were not significant (g = 0.173 and 0.071 respectively; both p≥0.09). All data sets in this domain were homogenous (all p≥0.73; I2 = 0%). Output from the leave-one-out sensitivity analysis is shown in Table SV(O–Q).
Meta-regression
Meta-regression was performed on the effect size estimates from the combined body function domain and the duration of the exercise intervention (Fig. 3). The overall test of the model was not significant (Q(1) = 1.06; coefficient = –0.008; 95% CI –0.024 to 0.008; p = 0.30). In addition, the goodness of fit for this outcome was deemed significant (Q(20) = 87.810; p < 0.01), suggesting the dispersion of effects is outside the range expected from standard error alone. The analysis was conducted without (36), as the intervention duration by these authors far exceeded that of any other study and we believed it to be an outlier. Similar results were found for the activity and participation domain (Q(1) = 0.410; coefficient = –0.002; 95% CI = –0.008 to 0.004; p = 0.52; Fig. 4). However, goodness of fit was not significant (Q(8) = 2.310; p = 0.97).
Fig. 3. Meta-regression analysis of intervention duration (weeks) and the effect size (g) for outcomes within the body function component of the International Classification of Functioning, Disability and Health (ICF) disability framework. Each study (n = 22) is depicted by a circle, with the circle size representing the relative weight attributed to each effect size. Note that (36) was removed from the analysis due to the long duration of the intervention.
Fig. 4. Meta-regression analysis of intervention duration (weeks) and the effect size (g) for outcomes within the combined activity and participation components of the International Classification of Functioning, Disability and Health (ICF) disability framework. Each study (n = 10) is depicted by a circle, with the circle size representing the relative weight attributed to each effect size.
Publication bias
Possible publication bias was examined on the combined body function domain, each of the individual components, and the combined participation and activity domain. The funnel plot for the collated body function domain is shown in Fig. 5, where significant publication bias was identified using both the Begg and Mazumdar rank correlation test (Kendall’s τ = 0.299; p = 0.03 (1-tailed)) and Eggers linear regression method (intercept = 2.840; p = 0.01 (2-tailed)). Application of Duval and Tweedie’s trim and fill method indicated that 7 studies were missing to the left of the analysis (negative; implying that exercise interventions may impair outcomes within the body function component). These studies ranged from g = –0.233 to –1.276.
As outlined in Table III, there is limited evidence to suggest that exercise interventions are likely to have a debilitating effect on function (particularly up to the range shown statistically here). We consider it unlikely that such stark findings would have gone unpublished and, thus, have chosen to ignore this correction. However, even if the correction were accepted, a small beneficial effect on the body function domain still results (g = 0.175; 95% CI 0.046–0.303). Fig. 6 shows the funnel plot for the lower limb component of the body function domain, which also indicated significant publication bias (Kendall’s τ = 0.487; intercept = 2.100; both p ≤ 0.02). The analysis suggested that 4 studies were missing that imply exercise has a small-to-large negative effect on this component (g ranging from –0.113 to –1.333). Dissimilar to the commentary provided above on the combined body function domain, the correction results in the finding becoming non-
significant (g = 0.120; 95% CI = –0.037–0.277). However, as stated above, we believe it is unlikely that studies with such prominent contrary findings to the present analysis would not have been published and thus, have chosen to ignore the corrected data. Publication bias was not evident for each of the remaining components of body function or in the combined activity and participation domain (all Kendall’s τ≤ 0.327; intercept≤ 2.839; all p≥0.08).
Fig. 5. Funnel plot of the combined body function domain. The included and imputed studies are denoted by the white and black circles, respectively. Studies reported to the right of 0 represent exercise interventions having a positive effect on the respective domain and/or component.
Fig. 6. Funnel plot of the lower-limb component of the body function domain. The included and imputed studies are denoted by the white and black circles, respectively. Studies reported to the right of 0 represent exercise interventions having a positive effect on the respective domain and/or component.
This systematic review summarizes the role of exercise for muscular strength and cardiovascular fitness in polio survivors. The 21 studies were grouped into respective ICF domains and/or components based on the ICF codes (40) and administered to quantitative synthesis. The overall results for the body function component (motor function, cardiovascular, mental and sensory domains) show that interventions have an effect favouring improvement in the body function of polio survivors. Results indicating improvement were also found for measures of activity and participation related to exercise. These findings provide clarification for a 2008 meta-analysis, which questioned the inclusion of muscular strengthening interventions in research (10), and build on the conclusions of the 2010 and 2011 reviews that stated that rehabilitation interventions seemed effective (14, 41).
Study heterogeneity and quality
Heterogeneity varied among the findings of this study. Although some findings were homogeneous (the combined activity and participation components), most findings displayed moderate to substantial heterogene-ity, which remained following sensitivity analyses. This may be explained by when this set of studies was published (all since 2001), in relation to the emergence of the ICF framework (2001), which oriented re-searchers to human functioning, resulting in more frequent inclusion of activity and participation measures. These studies were also of a higher quality: scoring 71+% (Table SIV) except for one (31) (at 59%). In addition, we observed a difference in quality (based on our assessment using a reduced Downs and Black checklist (15), when comparing studies published before and after 2001. Studies in this review published since 2001 appeared to be of higher quality, when assessed using this quality appraisal checklist.
International Classification of Functioning, Disability and Health
The results were presented in ICF components and domains, to enable meaningful interpretations to be made in a familiar framework of disability. The body function component is split into domains of motor func-tion, cardio-vascular fitness, and mental and sensory, enabling
the key topics of this review to be discerned. The activ-ity and participation components’ domains are combined, as each is oriented to the performance of tasks. Combining these latter 2 domains can provide context for potential positive outcomes and prognosis for social independence (40). The Core Set for PPS proposed by Bocker et al. (2016) helped to narrow the ICF cate-gories, providing clearer directions for assessment and documentation in clinical practice and research (17). This was an overall strength of this review outlining the effectiveness of muscular strengthening and aerobic fitness activities across a range of domains (e.g. body function – cardiovascular d450: walking), while still allowing specificity to individual outcome items (e.g. 6-min walk test as measure of fitness).
Intervention duration
Studies ranged in duration from 5 to 32 weeks. The meta-regression analyses of intervention durations vs effect (Figs 3 and 4) excluded the 2-year study (36), which was an outlier that skewed the regression line. This study (36) showed the strongest effect size amongst the studies, suggesting continued gains in the long term could be established in focal muscle groups when a non-fatiguing protocol is established in-clinic and continued as a home programme. Particularly able, motivated, and resourced polio survivors may have been recruited in this study, possibly lowering the attrition risk and biasing the outcomes. Current evidence seems to suggest progression of symptoms may not be as rapid as anticipated (8); however, without further long-term studies, it is difficult to confirm the rate of deterioration or the maintenance of key gains in the active population.
The body function domain analysis shows the dominant cluster within the remaining studies being between 4 and 16 weeks of intervention, this is reflective of interventional exercise studies, which look for measurable effects within several months. A similar analysis for activity and participation domains (Fig. 4) shows a weak overall regression line. Both sets of domains had an apparent negative (waning) effect slope in response to duration. A subtle gradual worsening of symptoms amongst participants may explain this effect slope, or the protocols may not have managed fatigue adequately. Polio survivors can be affected by fatigue within and between sessions, and serially. We recommend exercise protocols that acknowledge and limit fatigue, concurrent with education on fatigue management, with the aim of improving long-term motivation and adherence to exercise.
Effect sizes
Small-to-moderate improvement effects due to exercise interventions were seen in the motor function components and mental and sensory domain, while effects that appeared to be of clinical interest were identified in the cardiovascular component (not significant) and activity and participation domains, as outlined in Table III.
Although the effect sizes were modest, clinicians and polio survivors should derive confidence from further evidence of exercise favouring improvement across a range of contexts. What might be most reassuring, is that the strongest exercise effect was in outcomes within the mental and sensory domain (outcomes
related to pain and fatigue) favouring improvement in 2 highly prevalent symptoms in post-polio conditions. This challenges the findings of an earlier systematic review and meta-analysis (10), identifying no associations between exercise and improved fatigue management, and may be due to the increased number of studies included in the current research.
Body function domains
Motor function component. A prominent component of polio sequelae is increasing weakness across muscle groups (4). Exercise can be perceived by polio survivors and clinicians as disadvantageous to maintaining func-tion, due to discerning effects such as pain and fatigue. Long-term stress on polio-surviving motor units is widely accepted as precipitating muscle weakness through the degradation or loss of these motor units (10). Among the studies examined in the current analysis, strength outcom-es in 5 studies (31, 33, 34, 38, 39) had limited effects on either improvement or impairment. This demonstrates the need for further high-quality mode-testing studies to discern intervention modes with potential adverse effects across LEoP and PPS populations.
In their 2016 article, Vroon et al (9) discuss nuances of strength and cardiovascular exercise prescription in this population: anaerobic threshold as a tolerance limit, musculature chronically utilised being adapted to higher loading, the limitations of non-whole body exer-cise, and individualization (14). We agree that these factors are significant contributors to the heterogeneity of results within studies on polio survivors, and need to be balanced against participation outcomes.
Exercise prescription criteria for polio survivors engag-ing in strengthening activities, such as those summaris-ed by Gonzalez et al. in 2010 (14), should be utilised. Most studies in this analysis excluded candidates with severe weakness or excluded individuals’ muscle groups with a manual grade of less than 3/5. Further, studies highlight the importance of monitoring and responding to person-specific limits or adverse events during interventions with individualized modifications (5, 29). Without applying itemized criteria to set exercise participation limits, harmful or null overall exercise effects may arise in this population (5). It is essential that clinicians adhere to these tenants (prescription and exclusion) of exercise when treating polio survivors. The variety of measures and muscle groups strengthened effectively and safely across the included studies in this review indicates that strength exercise is suitable for polio survivors; a finding that is consistent with previous literature (10).
Cardiovascular component. The criteria of included
studies allowed a broad range of assistive device use, limb bracing use, and fatigue profiles amongst participants. Exclusions usually reflected the physical requirements of the cardiovascular intervention mode and the severity of existing weakness. Barriers to polio survivors maintaining or improving cardiovascular fitness include: global and peripheral fatigue, muscle weakness profile, use of assistive devices, activity choices, and the risk of falls (29). Thus, an individual’s profile determines the feasibility of fitness exercise mode.
Clinically, exercise mode decisions should be similarly based on polio survivors’ ability and symptoms, accommodating any evident body limitations and assistive technology use (5). The studies incorporating cardio-vascular domain interventions used combinations of limb use, body position and interface. This demonstrates polio survivors’ tolerance of a variety of cardiovascular exercise modes already available in clinical settings.
Mental and sensory component. The results of this review indicated links between muscle strengthening exercise and mental and sensory component, particularly fatigue (36% of the mental and sensory measures report-ed in the included studies). Fatigue is multidimensional and complex, and the measures used in the included studies (FSS, FIS, MFI-20, VAS) are non-specific to body system or condition (32). Fatigue is a pervasive symptom amongst polio survivors and is more prevalent than weakness (5). We recommend that consistent use of the fatigue measures should be used with polio survivors in research and clinical settings, and strict muscle pain and fatigue avoidance protocols should be adopted as demonstrated, consistent with previous protocols outlined in the literature (36, 42). In contrast, pain measures accounted for 19% of the mental and sensory measures reported, a representation much lower than expected, as it is important to monitor pain during exercise so that symptoms of pain or soreness in the polio survivors involved are not excessive (2). The presence of only one mental and sensory weakness measure among the included studies may be explained by the abundance of objective motor function testing measures performed. The inclusion of subjective weakness as a mental and sensory evaluation measure could capture the lived experience of functional strength during activity and may add scope to studies of non-motor oriented post-polio conditions (43).
Limitations
This systematic review and meta-analysis address-ed limitations across the literature regarding polio
survivors exercising and previous meta-analyses, such as (10); there were a number of points of improvement. A key assumption of the analysis carried out was that independent studies were unique cohorts. This was not the case in 2 examples: subjects in (22) were recruited from the cohort of 12 subjects originally studied in (23). Similarly (9) followed the same cohort as (3). Furthermore, our systematic search of the literature only included studies available in English; hence, we recommend that future reviews include languages other than English within searches, particularly given contemporary translation options outlined in the Cochrane Handbook (19). It is possible that such studies could influence the publication bias highlighted in this review. Further research into more individualized approaches to exercise prescription for polio
survivors would greatly advance research in this area.
The findings of this review and analysis provide “very low level evidence” (according to the Grading of Recommendations Assessment, Development and Evaluate; GRADE) to polio survivors, clinicians and researchers. The main findings of this review relate specifically to changes in body function, and activity and participation, and include evidence of effect on improved functioning without furthering debility in polio survivors. This systematic review and meta-analysis provides additional insights into effects associated with exercise, across various types of interventions, in polio survivors, and advances the level of methodological quality of research in this area. Although there was evidence demonstrating effect across domains, due to inherent biases within the literature to date, further and high-quality primary exercise-
focused research is required in order to strengthen the certainty of evidence regarding important research questions about the ongoing health of polio survivors.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize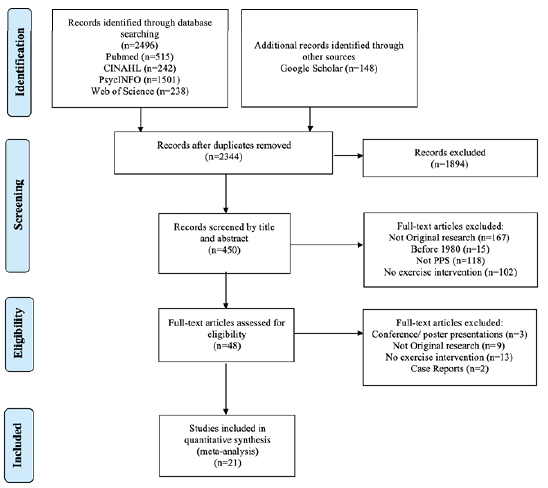 Click to show fullsize
Click to show fullsize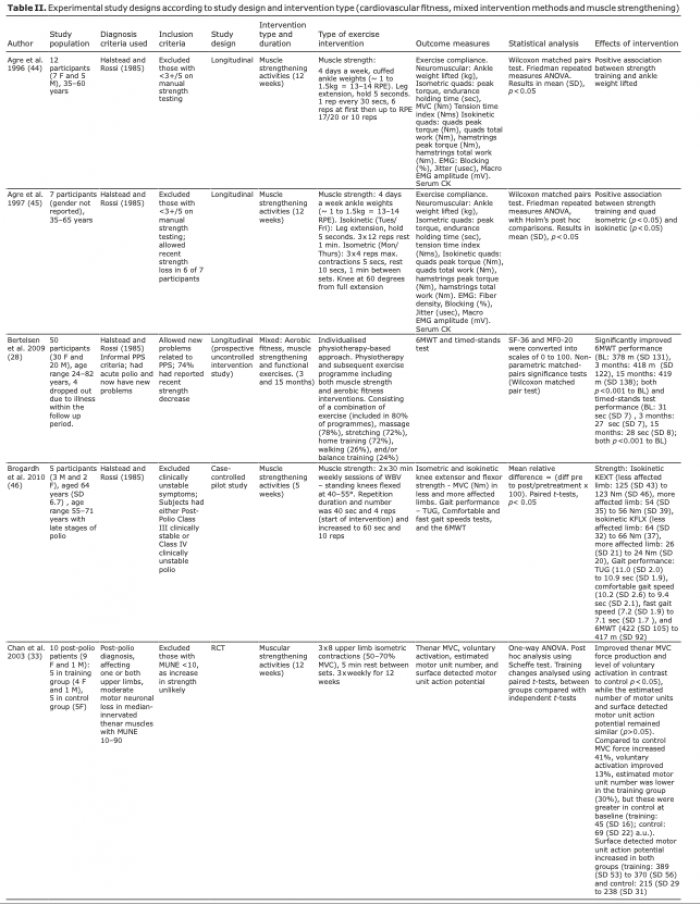 Click to show fullsize
Click to show fullsize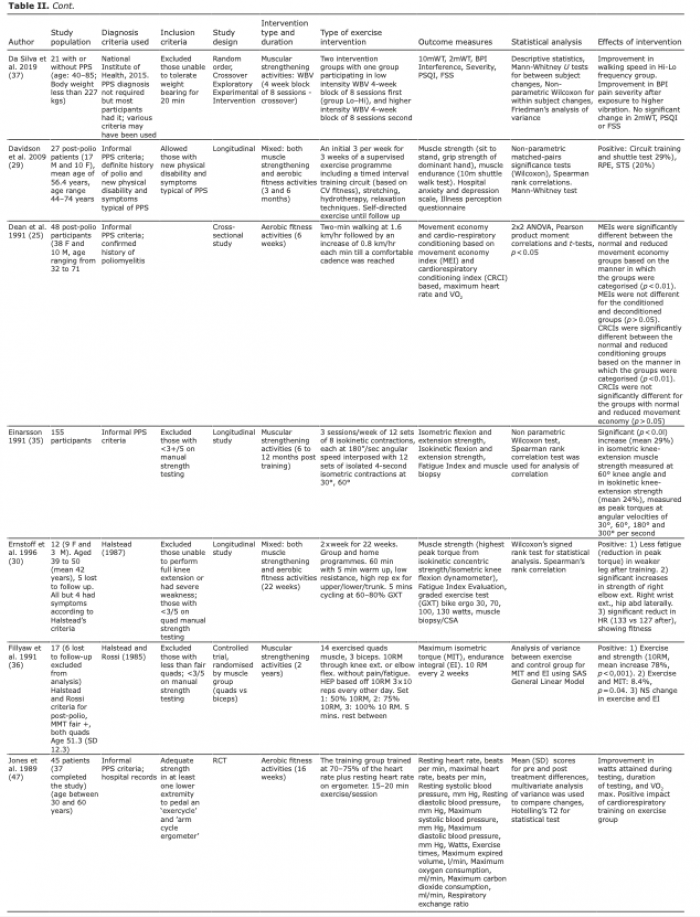 Click to show fullsize
Click to show fullsize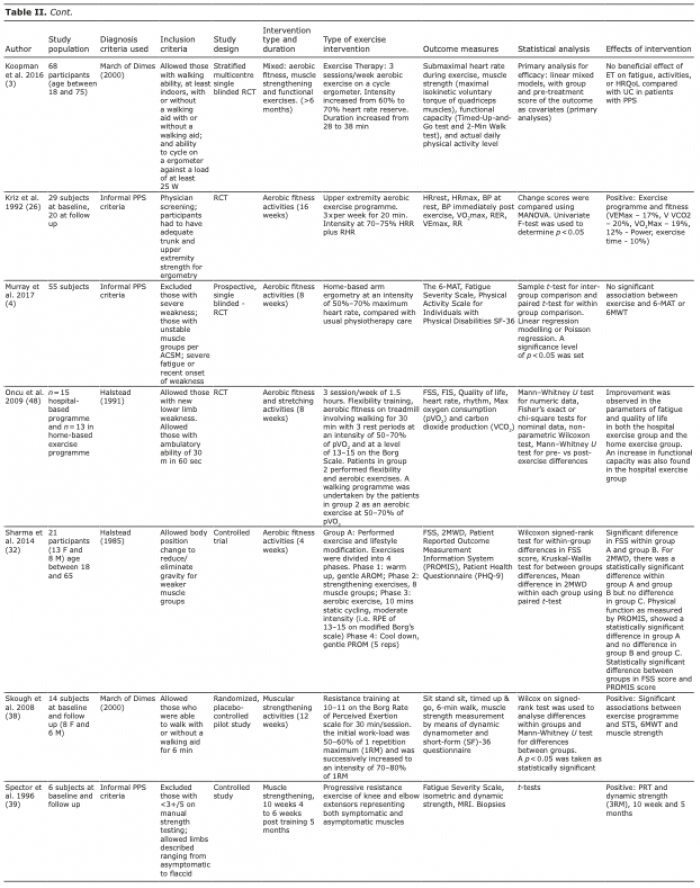 Click to show fullsize
Click to show fullsize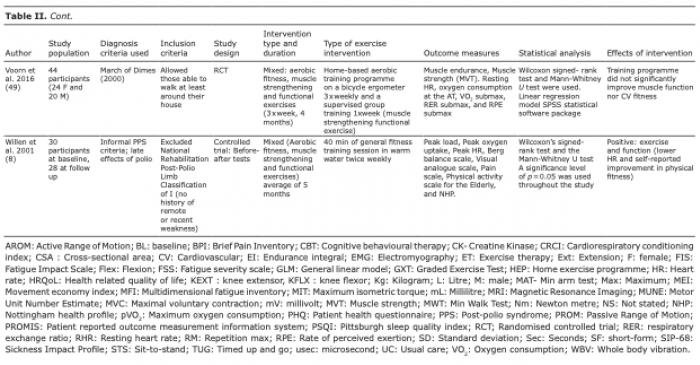 Click to show fullsize
Click to show fullsize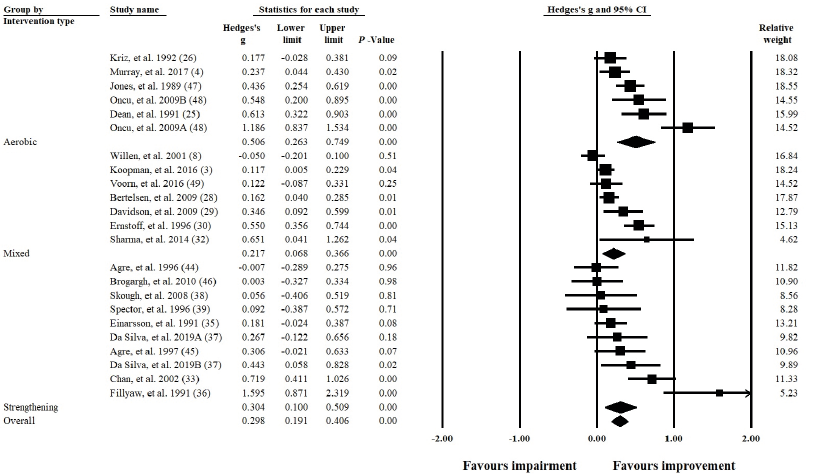 Click to show fullsize
Click to show fullsize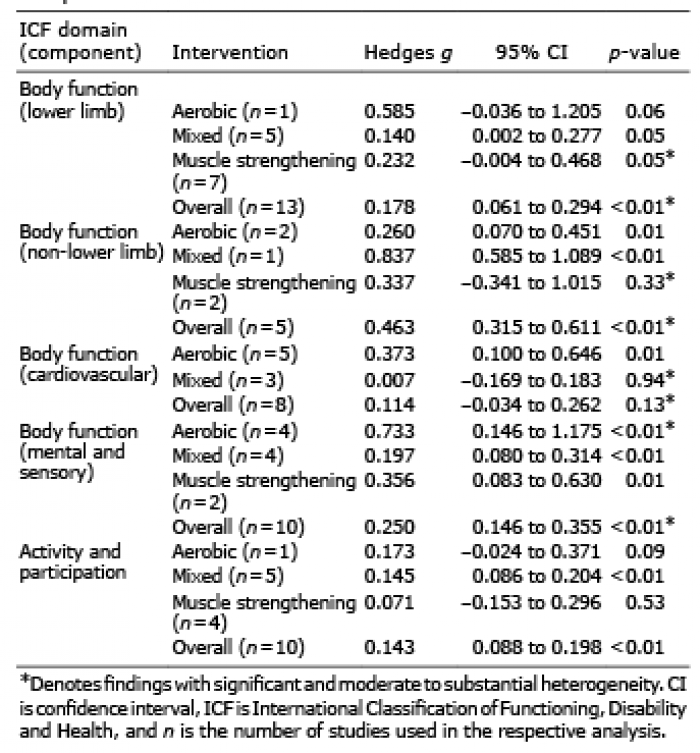 Click to show fullsize
Click to show fullsize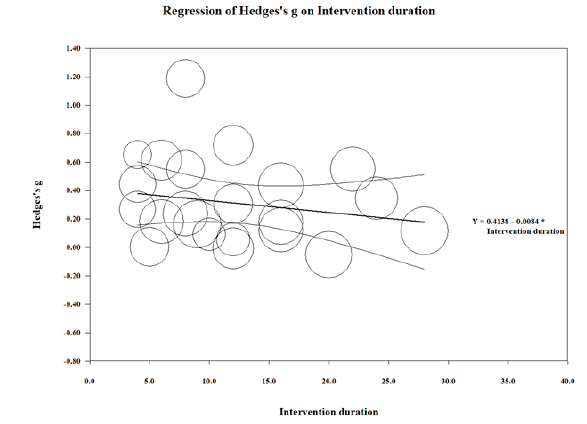 Click to show fullsize
Click to show fullsize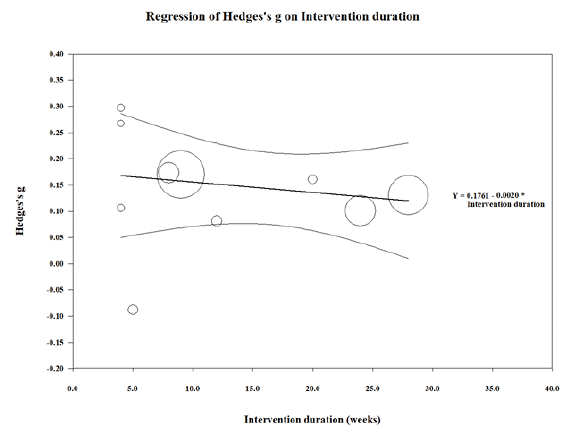 Click to show fullsize
Click to show fullsize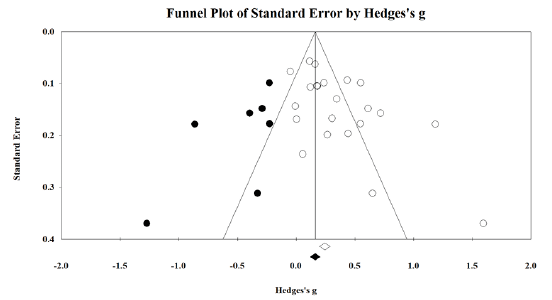 Click to show fullsize
Click to show fullsize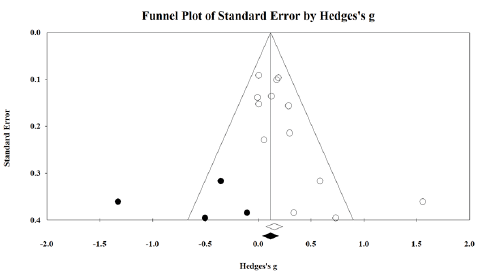 Click to show fullsize
Click to show fullsize